AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2692-9562/025
*Corresponding Author: G Buiret, Service d’ORL et de chirurgie cervicofaciale, Centre Hospitalier de Valence, 159 Boulevard du Maréchal Juin, 26953 Valence.
Citation: A Guillemaud, G Buiret, M Fieux, S Zaouche, JC Lifante. (2021) Assessment of voice changes of patients after thyroidectomy without inferior and superior laryngeal nerves injury according to the intraoperative neuromonitoring. 3(2); DOI: 10.31579/2692-9562/025
Copyright: © 2021, G Buiret. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 23 February 2021 | Accepted: 26 April 2021 | Published: 02 July 2021
Keywords: thyroidectomy; inferior laryngeal nerve; superior laryngeal nerve; voice quality
Objectives: to assess voice changes of patients after thyroidectomy without inferior and superior laryngeal nerves injury according to the intraoperative neuromonitoring.
Material and methods: This monocentric study included all patients who underwent thyroidectomy with laryngeal nerves neuromonitoring between September, 2018 and December, 2019. The voice assessment was performed 1 month before and 3 months after surgery. It was both subjective (with Voice Handicap Index 10 and GRBAS scale) and objective (Dysphonia Severity Index). Voice was considered impaired if there was an increase ≥ 4 points of the Voice Handicap Index 10 score or ≥ 1 point of the GRBAS scale score or a decrease ≥ 2 points of the Dysphonia Severity Index score between the two vocal assessments. A composite score was created, combining both subjective and objective scores. Predictive factors of altered voice were seek.
Results: Fifty-nine patients were analyzed. Mean Voice Handicap Index 10 varied from 3.39 ± 5.40 to 2.90 ± 5.29 (p = 0.62) before and after the surgery respectively, mean GRBAS from 0.64 ± 0.76 to 0.73 ± 0.85 (p = 0.57) and mean Dysphonia Severity Index from 8.47 ± 1.15 to 8.31 ± 1.03 (p = 0.42). Voice impairment composite score identified 14 patients with an impaired voice (23.7%). Age ≥65 years, preoperative Voice Handicap Index 10 score ≥ 3 and thyroidectomy past history were independent risk factors of voice impairment.
Conclusions: the voice quality 3 months after thyroidectomy was not significantly subjectively and objectively changed compared to before thyroidectomy. When grouping voice impairment scores, age ≥65 years, preoperative Voice Handicap Index 10 score ≥ 3 and thyroidectomy past history were independent risk factors of voice impairment.
In France, 49 477 thyroidectomies were performed in 2014 [1]. The main and specific risk of this procedure is post-operative dysphony [2]. This procedure may be explained by a lesion of the lower laryngeal nerve resulting in vocal alteration by paralysis of the ipsilateral vocal cord. This complication incidence is estimated between 0 and 18.6% for an average value of 2.3% [3]. In the absence of injury to this nerve, post-operative vocal changes are regularly attributed to damage to the External Branch of the Upper Laryngeal Nerve (EBULN), whose incidence is estimated between 5 and 28% of thyroidectomies [2]. This branch, innerving the cricothyroid muscle, allows the vocal cords to be stretched during phonation. In case of injury, the symptoms described are variable and not specific: limitation or loss of singing voice, vocal weakness, decreased maximum phonation time, reduction of voice strength [4].
It is possible to monitor the laryngeal nerves (neuromonitoring) during the surgery. This tool is reliable. Indeed, the negative predictive value of intraoperative monitoring of lower laryngeal nerves is very high, between 92 and 100% [4]. Thus, a patient operated on from thyroidectomy should not have a post-operative laryngeal paralysis if the electrical signals of these nerves are preserved at the end of the procedure. In addition, this laryngeal monitoring can be used to help identify and preserve EBULN [5, 6]. Stimulation of this nerve branch results in a glottic electrical response in 70 to 80% of cases [7]. However, the correlation between the absence of electrical (lower and upper) laryngeal nerves injury and quality of voice is not absolute and if the laryngeal monitoring allows to know post-operative cordal mobility, it does not guarantee the absence of alteration of the patient's vocal quality. Indeed, other causes of post-thyroidectomy vocal impairment are classically advanced: laryngeal edema, any other post-intubation complication, muscle lesions (section or resection of an infrahyoid muscle, lesion of one cricothyroid muscle), changes in the vascularization or the lymphatic drainage of the larynx, post-operative pain itself, psychological impact of this surgery or hormonal changes secondary to the thyroidectomy [8].
Few studies focused on the evolution of the voice after thyroidectomy in patients without laryngeal nerve lesion according to neuromonotoring. The main objective of this work was to analyze the evolution of patients' voices after thyroidectomy using subjective and objective tools. The secondary objective of the study was to identify predictive factors of voice impairment when intraoperative electrical responses were normal.
We conducted a single-center descriptive study from September 2018 to December 2019.
Recruiting
In the endocrine surgery unit, patients for whom thyroid surgery is scheduled has a consultation with an ENT one month prior to surgery to control laryngeal mobility.
All patients who volunteered during this period to receive a voice recording during this consultation as well as 3 months after surgery were analyzed.
The inclusion criteria were: patients ≥18 years-old, able to read French, and undergoing a thyroidectomy (partial or total, with or without associated recurrent or bilateral lymphadenectomy) with intraoperative monitoring of the lower and upper laryngeal nerves.
The non-inclusion criteria were: patients with preoperative laryngeal paralysis, an objectified cordal lesion at pre-surgical consultation or for whom an unrelated event interfered with speech-altering surgery occurred between preoperative consultation and surgery.
The exclusion criterion after surgery was the loss of the signal during lower laryngeal stimulation or the absence of a signal from one of the upper laryngeal nerves (true absence or missing signal data).
The study protocol was approved by the institutional review board and was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent before inclusion.
Population
Ninety-nine patients operated on from thyroid surgery received an ENT consultation with preoperative vocal check-ups. The flowchart of the study is shown in Figure 1. Among the eight patients with a lost of signal at the end of the surgery, only two had finally a laryngeal paralysis, all with thyroid carcinoma.

The mean age was 54 years ±14. The sex-ratio was 3 women per 1 man, the mean body mass index was 26.05kg/m² ± 4.68 and the mean follow-up time was 4 months. The population characteristics are presented in table 1.
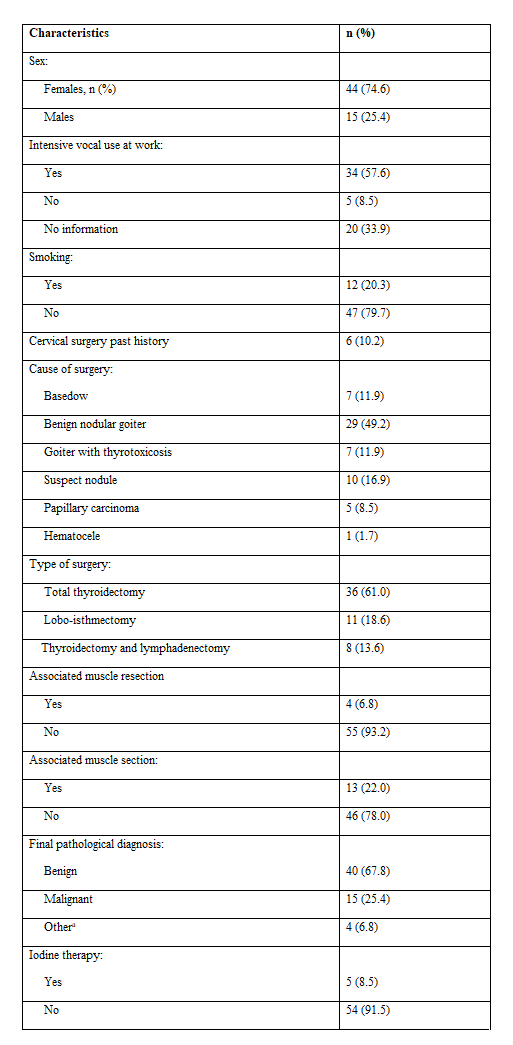
a Non-invasive vesicular tumour with papillary-type nuclei (n=3) and thyroid metastasis of a neuroendocrine tumour (n=1).
Surgical procedure
Nerve monitoring was carried out using Medtronic's NIM-Response 3.0 (Medtronic Xomed, Jacksonville, Florida, USA) in intermittent stimulation. The figure 2 presents the NIM and the expected reponses.
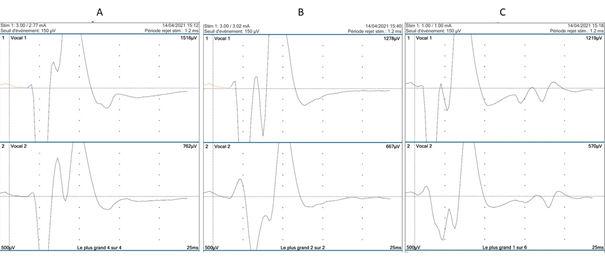
A: stimulation of vagus nerve before the inferior laryngeal nerve dissection; B: stimulation of vagus nerve after the inferior laryngeal nerve dissection; C: stimulation of the superior laryngeal nerve with collection of the signal of the inferior laryngeal nerve
The lower laryngeal nerve in the reseated lobe was considered functional at the end of the procedure if it was macroscopically intact and its stimulation direct to 1 mA as well as that at 3 mA of the ipsilateral vagus nerve resulted in a normal-shaped glottic electrical response (biphasic curve), intensity and latency on neuromonitoring. The EBULN was considered functional if its direct stimulation at 1 mA resulted in a glottic electrical response on neuromonitoring or if a contraction of the crico-thyroid muscle was observed with the naked eye.
If one of the four nerve branches (bilateral lower and upper laryngeals) was not considered intact, the patient was excluded from the study.
Voice assessment
The voice recording allowed subjective and objective analyses of the subjects' voices.
The subjective assessment of the voice was carried out by:
The objective assessment of the voice was made by an acoustic recording of the patient's voice. To do so, he/she was first asked to produce a [a] on his normal voice, without forcing, holding this phoneme for as long as possible. Then he/she was asked to perform an upward siren on a [or] few seconds in order to get the most acute voice possible. This recording collected the following data: the mean (Fo) and maximum (Fo-max) fundamental frequency in Hz, the maximum phonation time (MPT) in s, the Jitter (change in the average fundamental frequency on the [a]) in %, the Shimmer (variation of the fundamental intensity of the [a]) in % and the Harmonic/Noise Ratio (HNR). We have also chosen to use the Dysphonia Severity Index (DSI) [11] whose formula is calculated from the objective parameters for the study of the voice: DSI = (0.13xMPT) - (0.0053xFo-max) - (0.26xk) - (1.18xJitter) - 12.4. We chose to use a constant (k) as a minimum intensity for all patients (k =50 dB, classically encountered intensity). Indeed, we did not want the possible differences between pre- and postoperative DSI to be correlated only with the variation in intensity-minimum, a highly variable acoustic parameter. A poor quality voice leads to a DSI ≤ -5; a good quality voice ≥ +5.
All the variables were collected during the preoperative consultation and repeated three months after surgery.
The distribution of patients between normal and impaired voice was achieved after construction of a composite score. The voice was considered impaired if there was an increase of at least 4 points of the VHI 10 and/or an increase of at least 1 point of the GRBAS scale score and/or a decrease of at least 2 points of the DSI.
Statistical considerations
Comparisons of means were made using Wilcoxon test based on validation of the conditions of completion.
Comparisons of proportions were made by chi-2 tests.
The identification of predictors of voice quality was made by multivariate logistic regression after verification of the absence of colinearity and the stability of the model. Age was included in categorical form because of a non-linear relationship with voice quality.
A p<0.05 was considered significant. All statistical analyses were conducted using the R software (v. 3.5.3, www.r-project.org).
Comparisons of voice assessments before/after surgery.
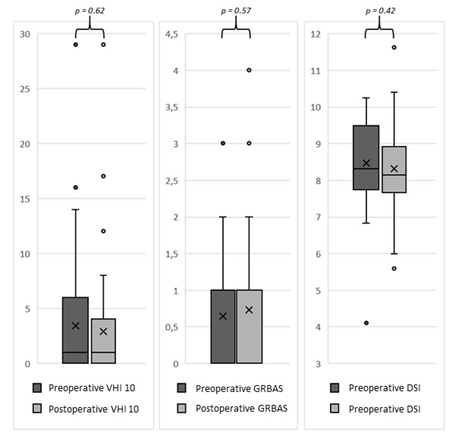
The mean VHI evolved from 3.39 ± 5.40 in preoperative to 2.90 ± 5.29 (p=0.62) in postoperative. The mean GRBAS score increased from 0.64 ± 0.76 in preoperative to 0.73 ± 0.85 in postoperative (p=0.57). Finally, the mean DSI evolved from 8.47 ± 1.15 before surgery to 8.31 ± 1.03 after (p=0.42).
The mean of the postoperative values of the 59 patients with the different acoustic measurements were not significantly different from those preoperative: Fo had evolved from 157.06 Hz to 164.01 (p=0.36), the mean Jitter from 0.66 to 0.54% (p=0.19), the mean Shimmer from 8.70 to 7.70% (p=0.19), the Fo-max from 495.35 to 471.93 Hz (p - 0.37) and the TMP from 15.56 to 14.19 seconds (p=0.19). Only HNR was significantly different in postoperative (15.31 ± 4.52 dB) compared to its preoperative measure (13.62 ± 4.36 dB) (p=0.04).
The figure 3 represents changes in scores at the VHI10, GRBAS and DSI scales of our population after thyroid surgery.
Of the 59 patients included, 12 patients (20.3%) answered in the affirmative to the question asked during the 3-month post-operative vocal check-up "Is your voice degraded compared to the pre-surgical one?"
Distribution of patients in altered/unaltered voice groups
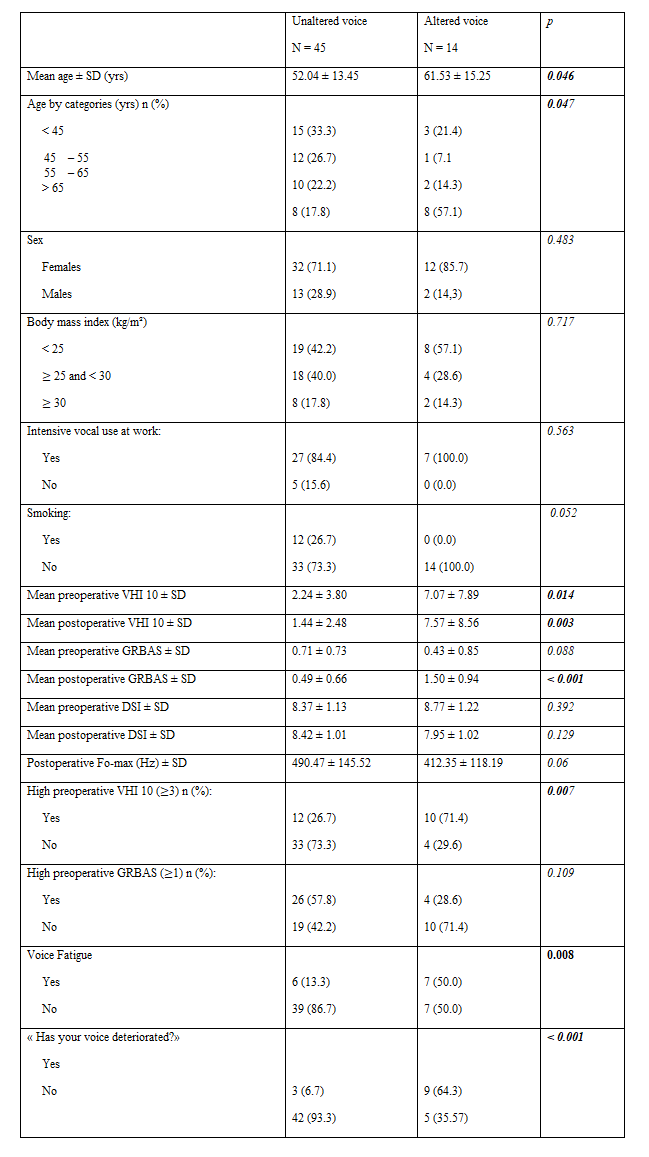
The distribution of patients using the composite vocal impairment score identified 14 patients with an impaired voice (23.7%) three months after surgery. Of these 14 patients, one met all three outcomes (VHI 10, GRBAS and DSI), one patient two of the three criteria (VHI 10 and GRBAS). The other 12 patients met only one criterion (one patient had an increase VHI 10 ≥ to 2, 10 an increase in GRBAS ≥ 2 and finally the last patient had a decrease in his DSI score ≤ 2). The characteristics of patients with and without voice impairment objectified by the chosen composite judgment criterion are listed in Table 2.
The other acoustic variables studied did not show a significant difference between the two groups (Fo, Jitter, Shimmer, MPT).
The surgical history, surgical indication, type of surgery, size of the larger thyroid nodule, resection or section of infra-hyoid muscles, pathological analysis and follow-up duration were not significantly different between the "unaltered voice" and "impaired" group.
Of the 59 patients included, 12 patients (20.3%) answering in the affirmative to the question asked during the 3-month post-operative vocal check-up "Is your voice degraded compared to the pre-surgical one?", 9 (75.0%) voice impairment objectified by the composite judgment test chosen in this work. The only patient with an alteration of his voice objectified by all the elements of the composite judgment criterion did not complain of having a "degraded" voice at 3 months of surgery compared to his preoperative voice.
In the group of patients who answered negatively to the question "Is your voice degraded compared to pre-surgical?", 5 (10.6%) of these 47 patients had vocal impairment using our composite endpoint as an endpoint. Thus, between these two groups, the difference in vocal alterations highlighted by the composite judging criterion was significant (p < 0>
Multivariate determination of predictive factors of altered/unaltered voice
Table 3 shows the results of the multivariate logistic regression model performed with age, sex, body mass index, preoperative VHI 10 score in categorical form, and type of surgery. Age ≥ 65 (Odds ratio (OR): 17,4; 95% Confidence Interval (IC) [1,6; 560,0], p=0.04), preoperative VHI ≥ 3 (OR: 9,5; IC [1.9; 66.4], p=0.011) and thyroid re-intervention (OR: 75,8; IC [2.1;9777.8], p=0.037) therefore emerged in our population as significant independent risk factors for vocal impairment.
Our subjective and objective study of the voice showed that the vocal quality at 3 months of thyroid surgery with a complete neuromonitoring response at the end of the surgery was not significantly impaired compared to the preoperative situation. Our composite judgment criterion identified 14 patients (23.7%) vocal impairment after surgery. The three independent risk factors for postoperative vocal impairment identified in our work were age ≥ 65 years, AHI 10 ≥ 3 in preoperative and thyroid reintervention.
Very few studies presented results with intraoperative monitoring of lower and upper laryngeal nerves in such a population with subjective and objective evaluation criteria [12-14]. Grouping three scores including subjective and objective evaluation variables allowed us to prioritize sensitivity to specificity. The vocal degradation might therefore be overestimated allowing us to identify patients with an altered voice, whereas it was considered to be of good quality by the averages at VHI 10, GRBAS and DSI scores analyzed separately. Among the risk factors identified in our model, age was also described by Sahli et al. [15], as well as thyroid reintervention [16]. Calcifications of laryngeal cartilage, alteration of the laryngeal lining, or atrophy of laryngeal muscles accompanying aging have all been suggestions advanced to explain that age is an independent risk factor for vocal impairment after thyroid surgery [17]. Other studies have shown that sex, body mass index, lack of use of laryngeal neuromonitoring, thyroid tumor size, thyroid gland weight or postoperative hypocalcemia were risk factors for altering vocal quality at a distance from surgery [18, 19], which we did not find in our work.
According to our composite score, 14 patients (23.7%) had altered their voices at 3 months of their thyroid surgery, which is classically found at a distance from thyroid surgery [2, 20]. However, unlike these studies, these vocal changes did not appear to be possible to be attributed to lesions of the lower or higher laryngeal nerves. To explain this large number of patients with altered voices but functional nerves according to the neuromonitoring, several reasons could be put forward (that can be limitations of our study). The combination of subjective and objective variables to detect impaired voices further improved sensitivity, compared to other studies using only subjective evaluation criteria may be one possible explanation [2, 8, 12, 13]. The short time between surgery and postoperative ENT evaluation at 3 months also overestimated the percentage of post-thyroid vocal impairment. This interval had been retained in order to minimize the number of patients lost of view. In addition, selection bias related to the inclusion of surgically operated patients in a referral hospital could explain this high percentage of impaired voices. Indeed, the preoperative mean VHI 10 was measured at 3.39, knowing that a normal VHI 10 according to the scientific literature is less than 2.83 [21]. However, we have shown that a preoperative VHI 10 ≥ 3 was a risk factor of vocal impairment. Thus our population did not have a voice considered normal in preoperative. Finally, the method of assessing the functional integrity of EBULN could be discussed. The electromyography of the cricothyroid muscle is the gold standard to ensure the proper functioning of the ipsilateral EBULN. However, this difficult-to-access technique is invasive and EBULN neuromonitoring at 1 mA, according to the scientific literature, is reliable for highlighting a complete nerve injury [7, 22]. But enough for a slight impairment?
No significant differences were found between the acoustic data before and after surgery other than an increase of HNR. This increase would even suggest an improvement in the patient's voice. Other studies have found alterations in Fo, Fo-max, Shimmer, MPT or but none monitored the EBULN [23, 24]. Thus, these acoustic changes could be attributed to damage to this nerve branch [25, 26]. The Engelsman et al. study monitoring the lower and upper laryngeal nerves did not object to any significant difference between the different acoustic parameters studied [14].
The perspective of this study is to find out if the voice impairment is linked with an EBULN injury that can’t be seen with the neuromonitoring or with another reason. Performing a perioperative electromyography of the cricothyroid muscle is too difficult but the technological improvement of the NIM with lower level of detection of the cricothyroid muscle May precise it.
In the absence of laryngeal nerve injury (lower and upper) objectified by intraoperative neuromonitoring, post-thyroidectomy vocal quality was not significantly impaired compared to preoperative. However, in our more sensitive model (combined score), 23.7% of patients undergoing thyroid surgery would have an alteration of their voice. The three independent risk factors for postoperative vocal impairment found in our work were age ≥65 years, VHI 10 ≥3 in preoperative and thyroid reintervention.
None
We would like to thank Drs. PEROUSE and COULOMBEAU (ENT) for their invaluable assistance in the acoustic approach to the voice and the paramedic team of the ENT consultation at the hospital for their contribution to the work of data collection.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
